
Airway management is a fundamental skill that all EMT’s and paramedics need to master. It’s been said that paramedics are great at two things, cardiology and airway management. That is quite true and providers need to “own” these important skills.
Airway management is vital to good patient outcomes. A poorly managed airway can have lasting effects long after the call. With aspiration and hypoxic brain injury being two of the most critical.
This article will not go into detail of how to intubate or bls airway management but will discuss three extremely important pieces of the airway management puzzle.

The three wise men consist of: a properly fitted BVM face mask, a properly sized oral pharyngeal airway, and a 10cc syringe.
A “hypothetical situation”…..
You’ve determined the need for airway management.
After committing to the airway you select an appropriate size oral pharyngeal airway, and place it using whichever technique your comfortable with. You begin ventilating the patient with an appropriately sized mask and BVM device. At some point the decision to manage the airway using an advanced device is made.
The conversation might go like this. “OK I’m ready to intubate. Stop bagging.” You remove the OPA and typically drop it in a random place..the floor, wherever. You pass the tube and inflate the cuff. As you’ve been taught you immediately remove the syringe, and that too goes wherever. Then you tell your partner to “bag”. They remove the face mask portion and drop that or toss it wherever and attach the device to the tube and ventilate so you can confirm tube placement. You ascultate bilateral breath sounds, no epi-gastric sounds, waveform capnography looks perfect. Tube is secured. Awesome job, Life is Good!
After making a couple of moves, like from the floor to the stretcher, and then to the ambulance your partner notices it is getting harder to ventilate the pt. (decreased compliance). No problem you say. You ascultate lung sounds and note decreased air movement on one side. Piece of cake, the tube migrated a little deeper all I need to do is slide it on back a bit. Where is the syringe…..DOH!!! “Where’s my ALS bag??!!!” Crap crap crap……
Or you make a few moves and this time you lose the waveform tracing, SPo2 is 80%. GRRR…must have extubated. I know what your thinking, great now we have to go through the entire intubation sequence again. “I’ll pull the tube”, “you bag em’ back up.”
“Hand me the syringe to deflate the cuff” “You can’t find it?!!” “What do you mean you don’t know where the mask went?””Just grab another one out of the cabinet.” “Hey it’s hard to bag.” GRRR….”where’s the OPA?” “Found it here on the floor.” “It’s all cruddy, what do you want me to do?” “Just grab a new one.”
SPo2 is 70%, crap crap crap………”Wheres the OPA” “All I can find are too small or too big.” “What do you want me to do?”
Sounds like one or two wrong moves have turned this into “one of those calls” the wheels have come off and now we’re behind the eight ball so to speak. A poor patient outcome is a very real possibility.
How do we avoid these disasters?
I’m a huge proponent of compartmentalizing each skill. By that I mean take each skill you are going to perform and assemble ALL of the required pieces before you commit. “Build” a workstation within easy reach. It is absolutely OK to use a “check list”. After enough time and experience most of these skills will become second nature. Muscle memory plays a large part, but you must be able to think on the fly as problems arise, and they always do. Having an organized approach to each skill helps immensely.
Airway Management Check-List
- Oxygen, enough in the tank? Delivery device?
- Properly sized BVM and face piece.
- Oral airway, nasal airway
- Suction, does it work? Tubing and hard or soft suction available?
- Laryngoscope and blade
- ETT, plus one size higher and one size lower
- Stylet or Bougie
- 10cc syringe
- Rescue airway device (King, LMA, Combi)
- Commercial tube securing device
- End tidal capnometry device
- Stethescope
Note the first items are typically where airway management starts, then you move into the invasive part of placing the tube, and finally to confirming and securing.
There are a number of these online. A quick Google search will get you plenty of examples.
Check out this one on EMCRIT
Post intubation
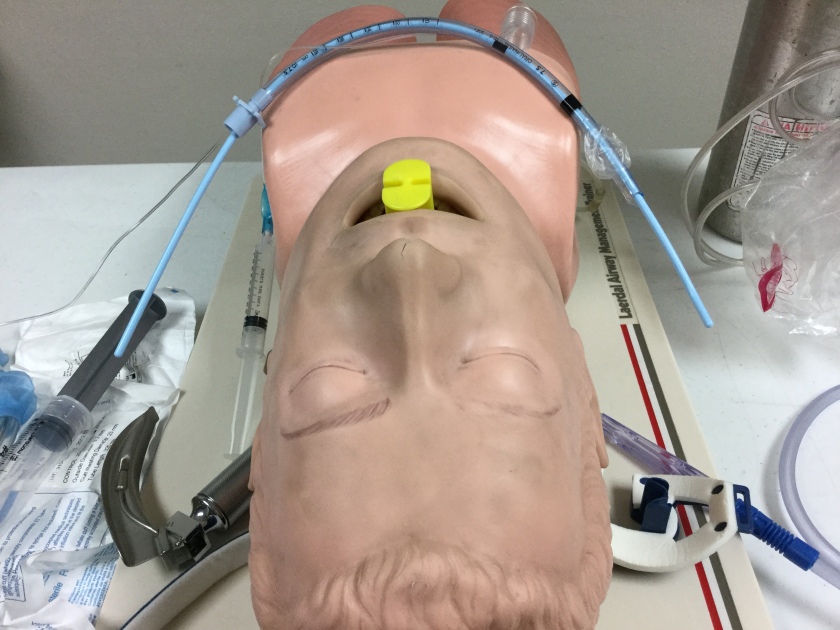
Remember “A hypothetical situation” a few paragraphs ago? Where did all of the pieces that were used and no longer needed wind up?


The photos show one option to keep all three pieces together and within easy reach. You could also place them in your airway roll (contamination problem?) next to the air chair on the shelf. Whatever works best for you, with the main point being to keep them together and available.
The take away’s
- Practice practice practice…..not until you get it right, until you can not get it wrong!
- Develop your skills and knowledge
- Use a check list when performing procedures
- Use “workstations” to assemble your equipment
- The less you need to think about the skill, the more mental muscle left to deal with a changing situation
Fine Print
The ideas, thoughts, and concepts presented are the opinion of the author. When providing any care follow your state, local, and agency protocols and guidelines.
